The delinquency rates aren’t new. Detroit is a shrinking city with lots of poor residents left behind. The city is bankrupt. The aggressive enforcement measures towards those behind in their bill is new. City management official claim that the water and sewer utility has been plagued by corruption, incompetence and inadequate maintenance for decades, and is seriously in debt. The utility’s bond rating is Baa with $5.4 billion in bond obligations. Moody’s Financial Ratio Analysis places the utilities debt ratio at around 90%.
Detroit is currently run by an appointed emergency manager selected by the Governor under a controversial new Michigan law. The emergency manager supersedes all elected authority in the city and has nearly absolute power. Pressure to shut off delinquent residential water customers comes under his authority.
To understand Detroit’s situation it is helpful to step back first and look more broadly at water utilities here and abroad.
Water Utility Rates are on the Rise
A 2000 survey by the U.S. Census Bureau found that, “The average annual cost of water and waste water for a household that pays directly for service is $476 per year, ranging from $334 in Nebraska to $721 in Hawaii.” That figure works out to about $40 per month while an EPA website says: “American household spends, on average, only $523 per year on water and waste water charges… ” That works out to a U.S. average of $43.58 per month for water and sewer.
In a recent USA TODAY article entitled “Nation’s water costs rushing higher” it was reported that:
“While most Americans worry about gas and heating oil prices, water rates have surged in the past dozen years, according to a USA TODAY study of 100 municipalities. Prices at least doubled in more than a quarter of the locations and even tripled in a few.[snip] Monthly costs topped $50 for consumers in Atlanta, Seattle and San Diego who used 1,000 cubic feet of water, a typical residential consumption level in many areas.
There is also a water and sewer industry report prepared in 2012/2013 by Black and Veatch, a private firm. This report says the cost of water in Seattle, for example, was $8.19 per 1.000 gallons, not including the sewer charges. The combined monthly bill for sewer and water in Seattle was $177.93 per month for residential customers using 7,500 gallons, according to this report.
Meanwhile in Detroit, according to the Black and Veatch report, the monthly water and combined sewer and water rates for residential customers using 7500 gallons per month was $24.12 and 70.89 respectively. So which figures are correct?
It turns out that water and sewer utility prices are deceptively difficult to understand or to compare from city to city. There are different units of measurement, different seasonal schedules, peak and off-peak metering and different rate structures. Also, in cities especially, water and sewer rates are separately billed but inseparable because water use is the measure of sewer use in most cases. Billing is combined. Sewer rates are generally higher, often double the water rates. Comparing water pricing without including sewer pricing can be very misleading. Finally, to get a full picture of a municipal utility overall, it is important to compare the rates for commercial water/sewer uses and the wholesale rates the utility charges industries.
An Apples to Apples Comparison
The table below directly compares the published water and sewer rates for Detroit and Seattle (converted to dollars/1,000 gallons). Seattle was selected for comparison because it was one of the cities mention in the USA Today article as having the highest rates. The data is from both city websites.
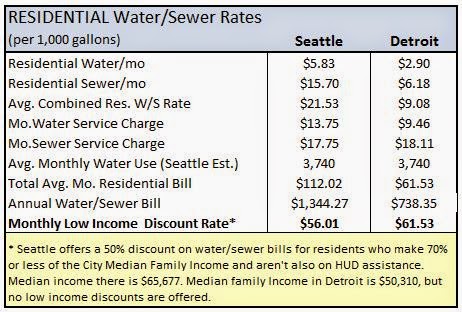
Detroit, a city with a median family income 25% lower than Seattle, has flat rates. It offers no low income discounts. As a result, the average low income water/sewer bill in Detroit is higher than in Seattle.
To complete the look at water and sewer utilities in these two cities it is important to compare rates for retail commercial and wholesale water customers as well. The information on the websites is a little more difficult to extract in this area. The graph below is my best attempt.
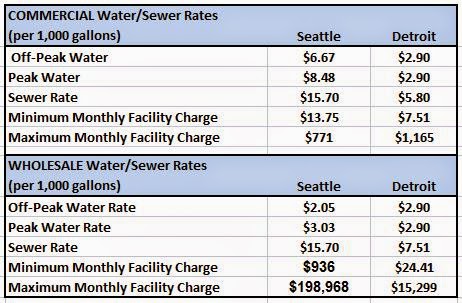

What jumps out here is the different rate structures in these two cities. Commercial rates in Seattle are somewhat higher than in Detroit, the monthly minimum and maximum wholesale facility charges are significantly higher. Seattle also has a peek commercial water rate that is higher than off-peak to encourage conservation. Meanwhile the difference in the maximum and minimum facility charges in the two cities is 13 times and 38 times higher in Seattle. This suggests that there may be some latitude for Detroit to raise commercial and wholesale water/sewer utility rates to help offset the current financial short fall. Additionally, the Detroit utility could also consider raising residential rates for customers who can afford the increase and discounting rates for low wage earners, as Seattle does.
In the meantime, Detroit should look at the creative collection alternative already practiced in other states and try to find effective alternatives to shutting off water to so many of the residents they are honor bound serve. Access to water is an essential human right and cutting off resident from water should be a last resort. Just reviewing the rate structure suggests possibilities that may not have been considered yet.
A Global Perspective
How do U.S. water rate compare with the cost of water in other cities around the world?
The Organization for Economic Co-operation and Development ( OECD ) conducted two surveys of residential water tariffs in 1999 and in 2007-08, using a reference consumption of 15 cubic meters per household per month. The 2007-08 survey covered more than 150 cities in all 30 OECD member countries. The survey does not claim to be representative. The OECD survey was complemented by a survey of the industry information service Global Water Intelligence (GWI) conducted in 2007-2008 in parallel with the second OECD survey. The 2008 GWI survey covered 184 utilities in OECD countries and 94 utilities in non-OECD countries. GWI has repeated its survey every year from 2009 to 2012, increasing the number of utilities surveyed to 310 in 2012.
When you convert the OECE findings to US gallons the results indicate that the average water rate in the 310 global cities surveyed is $7.50/1,000 gallons. The range of water rates vary greatly from $0.11 per 1,000 gal. in Saudi Arabia, to $34.86 per 1,000 gal. in Denmark. Then there are also countries, such as Ireland, where water is delivered to households free of charge.
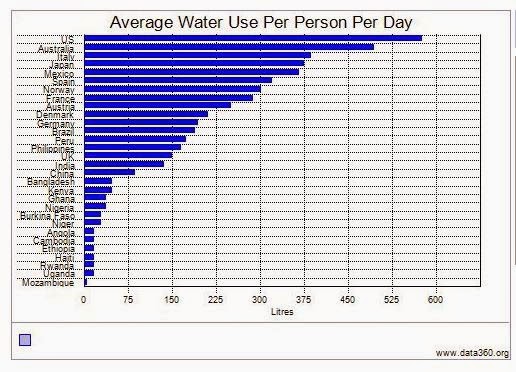
The benchmark for monthly water use in the OECD survey was 15 cubic meters per month, or 3,963 gallons per month, compared with 7,481 gallons per month in the United States. As the graph below shows, U.S. households use more water than do households in most other countries. In the examples above, the difference represents an 88% higher rate of water use in the U.S.

To complete the comparison it is important to acknowledge that higher volumes of water used per household in the US lowers the cost per gallon. In the USA TODAY article, greater conservation of water by customers was named as one of the reasons for higher water rates. When you factor in the average water use in the US with the benchmark estimate of average monthly use in the OECD study, residents in Atlanta, Seattle and San Diego are paying approximate $50 per month for water while residents in foreign cities are paying about $30 per month.
If U.S. water consumption dropped to the lower global levels, residents in the cities mentioned above would pay about $27 dollars per month. However, lowering water use that much in the U.S. would significantly raise the cost per gallon. There are so many variables and assumptions in all of the underlying data that this is a rough guess.
Keep in mind also that the cost of water for the data cited here is for cities, yet it isn’t clear if the figures given include sewer costs. The quality of sewer systems and their associated costs vary greatly, both nationally and across the globe. The best that we can gather from this very rough comparison, then, is the impression that current water rates in the U.S. are somewhat comparable with average global rates.
Water is an essential part of our daily life and a human right. It is a finite resource that is growing in scarcity. Social and environment forces are combining to raise water prices everywhere. The trend in rising prices is likely to accelerate as U.S. water conservation become more essential to meet our basic water needs, and this article doesn’t even touch on agricultural where most of our water is used. With scarcity comes increased commercial opportunities and there will be growing pressure to privatize municipal water utilities for profit. Balancing commercial interests with human needs and human rights is a conversation we need to have. Increasing public awareness is critically important for our future and the media will need to do more and better reporting to inform the public.