Home » Posts tagged 'Child Welfare'
Tag Archives: Child Welfare
Heart of the Matter
by Brian T. Lynch, MSW
I knew a boy once who had a long red mark on his neck that someone thought was from physical abuse by his father. I talked to the boy. When I asked how he got the mark on his neck, he fell silent. Then he motioned for me to follow him.
He brought me outside to a shed in the back yard and opened the door. He pointed to a piece of rope on the floor and said,”I tried to hang myself, but the rope broke,” I put my hand on his shoulder as we both just stared at the rope.
I went back to the house to speak with his dad, The man clearly loved his son. He said he just wanted his boy to grow up “the right way.” He admitted he yelled a lot, but said he would never touch is son because of the way his own dad had beaten as a child.
I asked the father to show me his scars from those beatings. He pointed to his heart and said, “They are all here inside me.”
“That,” I said, “is where your son’s scars are as well.” Then I told him how his son got the mark on his neck. The man called his son into the room, grabbed him in a hug and wept. The scars that harm us most are almost always the ones no one else can see.
Declaring War on the Poor
by Brian T. Lynch, MSW
Thom Tillis is now Senator elect from North Carolina, having beaten Democratic incumbent Kay Hagan in the 2014 election. During his campaign Tillis berated the poor and suggested that those people who can’t help being poor, like the truly disabled, should rise up and opposed welfare for the unworthy poor. What he actually said was:
“What we have to do is find a way to divide and conquer the people who are on assistance,”
North Carolina has 1.1 million poor. That’s 13.1% of its population. If these folks voted it would be hard to imagine Tillis getting elected, but Hagan and the Democrats have abandoned the poor and working class in this country as well. Now the poor are under attacks like this:
“We have to show respect for that woman who has cerebral palsy and had no choice, in her condition, that needs help and that we should help. And we need to get those folks to look down at these people who choose to get into a condition that makes them dependent on the government and say at some point, ‘You’re on your own. We may end up taking care of those babies, but we’re not going to take care of you.’ And we’ve got to start having that serious discussion.” – Thom Tillis
Watch for the U.S. Senate to put Tillis on the Health, Education, Labor and Pensions Committee to replace Kay Hagan. He is destine to become the chair of the Children and Families Sub-committee with his attitudes. His appointment would amount to a declaration of war on the poor.
So how should sensible people respond to divisive attacks like this on the poor and vulnerable? Should we begin making similar distinctions between the worthy and unworthy rich? Should we affirm those who earned their great wealth and provide social benefit but rescind all advantages given to those who use their inherited wealth to squeeze the people and their government for still more?
How we respond to these questions will define who we are as a nation.
Kids in Cages – Refugee Crisis at Our Border
by Brian T. Lynch, MSW
 It is It was Father’s Day and I was still haunted by story I hear about earlier this week. Over 70,000 children a year are coming across the US border from places like Guatemala, Honduras, El Salvador and Mexico, many of whom are unaccompanied minors. The United States is forced to house these children in temporary detention facilities under very difficult conditions. The situation is desperate as federal agencies and facilities designed to house adults races to accommodate the special needs of young children.
It is It was Father’s Day and I was still haunted by story I hear about earlier this week. Over 70,000 children a year are coming across the US border from places like Guatemala, Honduras, El Salvador and Mexico, many of whom are unaccompanied minors. The United States is forced to house these children in temporary detention facilities under very difficult conditions. The situation is desperate as federal agencies and facilities designed to house adults races to accommodate the special needs of young children.
On All In with Chris Hayes, José Diaz Balart reported about the humanitarian crisis at the US Mexican border. Unaccompanied minors are crossing the border in record numbers, sometimes as many as 300 a day. Some of these children are as young as 18 months old. But also, there are couples trying to cross the border with their children who are being met by members of Mexico’s drug cartel that take one of the parents hostages for ransom, allowing the other parent and children to cross into the States.
Balart also reported on the conditions that are creating these developments. One Guatemalan mother told him gang violence in her country is so bad that when their daughters reach puberty, gang members will come in and either rape them, kill them, or take them as their property. These parents feel they have no option but to send their children across the border to safety. When US officials try to interview young children to learn who their parents are it is not unusual for 4 and 5 years to not know their parents names or the name of the towns in which they lived. In some cases, trying to reunite children with their families is impossible.

While we flounder around once again in Iraq and other foreign lands with oil resources of interest, we are ignoring the deteriorating humanitarian situations in our own hemisphere. The immigration issues we face are usually couched in protectionist language when the root of the problem is really about promoting growth and stability in foreign countries much closer to home.
We need to direct more resources and attention on foreign aid and international diplomacy among our Latin American neighbors. The social and economic conditions in these countries have reach a crisis proportions. Our immigration problem is a massive refugee problem that our politics and the media isn’t addressing. The answers to real immigration reform fall well beyond the scope of our current political dialogue.
Obamacare – Is It For Good or Evil?
Like anything else, you can use a thing or abuse it. The Affordable Care Act is being shredded for political reasons in many states to create proof that it doesn’t work. It’s a shambles in the hands of those who want to use it as a cudgel with which to beat up Obama. More enlightened states are taking every advantage of the ACA and in doing so they are better serving their citizens and improving their state budgets. Here below is a snippet from an article in the Washington Post:
How we got Obamacare to work
By Jay Inslee, Steve Beshear and Dannel P. Malloy, Published: Washington Post, November 17, 2012
[snip] In our states — Washington, Kentucky and Connecticut — the Affordable Care Act, or “Obamacare,” is working. Tens of thousands of our residents have enrolled in affordable health-care coverage. Many of them could not get insurance before the law was enacted.
People keep asking us why our states have been successful. Here’s a hint: It’s not about our Web sites.
Sure, having functioning Web sites for our health-care exchanges makes the job of meeting the enormous demand for affordable coverage much easier, but each of our state Web sites has had its share of technical glitches. As we have demonstrated on a near-daily basis, Web sites can continually be improved to meet consumers’ needs.
The Affordable Care Act has been successful in our states because our political and community leaders grasped the importance of expanding health-care coverage and have avoided the temptation to use health-care reform as a political football.
In Washington, the legislature authorized Medicaid expansion with overwhelmingly bipartisan votes in the House and Senate this summer because legislators understood that it could help create more than 10,000 jobs, save more than $300 million for the state in the first 18 months, and, most important, provide several hundred thousand uninsured Washingtonians with health coverage.
In Kentucky, two independent studies showed that the Bluegrass State couldn’t afford not to expand Medicaid. Expansion offered huge savings in the state budget and is expected to create 17,000 jobs.
In Connecticut, more than 50 percent of enrollment in the state exchange, Access Health CT, is for private health insurance. The Connecticut exchange has a customer satisfaction level of 96.5 percent, according to a survey of users in October, with more than 82 percent of enrollees either “extremely likely” or “very likely” to recommend the exchange to a colleague or friend.
In our states, elected leaders have decided to put people, not politics, first.
[Read more here: http://www.washingtonpost.com/opinions/how-we-got-obamacare-to-work/2013/11/17/3f2532bc-4e42-11e3-be6b-d3d28122e6d4_story.html ]
_______________ … _______________
If you feel that the media isn’t doing a good job of covering the positive side this story and isn’t reaching the ACA doubters and haters you know, then do something about it. Point them to this article or refer them here to read something that is directly from the chief executives of states where the ACA is working.
Snippets: Toxic Stress and New Ways to Combat the Impact of Child Abuse and Neglect
What follows is a snip-it of an excellent article from the Opinionator section of the New York Times by David Bornstein. Within the article are hyperlinks to excellent source material on childhood toxic stress, its impact on children and new methods to prevent harm or treat children who are exposed to toxic stress. I have taken snippets of each of these hyperlinks to create an annotated index to the sources from Mr. Bornstein’s article. I hope that this will encourage further reading and understanding on this topic. Having spend 31 years as a social worker in child protective services it has been my experience that chronic and repetitive stress on children is both pervasive and incredibly damaging. It takes new protective service workers years of experience to recognize toxic stress and fully appreciate how damaging it truly is. The whole field of protective services is more oriented towards responding to physical abuse and acute safety risks than it is to chronic neglect or repetitive lower level trauma. – Brian T. Lynch, MSW
Protecting Children From Toxic Stress
New York Times – October 30, 2013
Imagine if scientists discovered a toxic substance that increased the risks of cancer, diabetes and heart, lung and liver disease for millions of people. Something that also increased one’s risks for smoking, drug abuse, suicide, teen pregnancy, sexually transmitted disease, domestic violence and depression — and simultaneously reduced the chances of succeeding in school, performing well on a job and maintaining stable relationships? It would be comparable to hazards like lead paint, tobacco smoke and mercury. We would do everything in our power to contain it and keep it far away from children. Right?
Well, there is such a thing, but it’s not a substance. It’s been called “toxic stress.” For more than a decade, researchers have understood that frequent or continual stress on young children who lack adequate protection and support from adults, is strongly associated with increases in the risks of lifelong health and social problems, including all those listed above.
[read more: http://opinionator.blogs.nytimes.com/2013/10/30/protecting-children-from-toxic-stress/?_r=0 ]
Toxic stress response: Occurs when a child experiences strong, frequent, and/or prolonged adversity—such as physical or emotional abuse, chronic neglect, caregiver substance abuse or mental illness, exposure to violence, and/or the accumulated burdens of family economic hardship—without adequate adult support. This kind of prolonged activation of the stress response systems can disrupt the development of brain architecture and other organ systems, and increase the risk for stress-related disease and cognitive impairment, well into the adult years.
When toxic stress response occurs continually, or is triggered by multiple sources, it can have a cumulative toll on an individual’s physical and mental health—for a lifetime. The more adverse experiences in childhood, the greater the likelihood of developmental delays and later health problems, including heart disease, diabetes, substance abuse, and depression. Research also indicates that supportive, responsive relationships with caring adults as early in life as possible can prevent or reverse the damaging effects of toxic stress response.
[read more: http://developingchild.harvard.edu/topics/science_of_early_childhood/toxic_stress_response/ ]
Centers For Disease Control and Prevention
http://www.cdc.gov/ace/index.htm
Survey shows 1 in 5 Iowans have 3 or more adverse childhood experiences
October 14, 2013By Jane Ellen Stevensin
Iowa’s 2012 ACE survey found that 55 percent of Iowans have at least one adverse childhood experience, while one in five of the state’s residents have an ACE score of 3 or higher.
In the Iowa study, there was more emotional abuse than physical and sexual abuse, while adult substance abuse was higher than other household dysfunctions.
This survey echoed the original CDC ACE Study in that as the number of types of adverse childhood experiences increase, the risk of chronic health problems — such as diabetes, depression, heart disease and cancer — increases. So does violence, becoming a victim of violence, and missing work days.
[read more: http://acestoohigh.com/2013/10/14/survey-shows-1-in-5-iowans-have-3-or-more-adverse-childhood-experiences/ ]
From the American Academy of Pediatrics
Technical Report
The Lifelong Effects of Early Childhood Adversity and Toxic Stress
- 1. Benjamin S. Siegel, MD,
- 2. Mary I. Dobbins, MD,
- 3. Marian F. Earls, MD,
- 4. Andrew S. Garner, MD, PhD,
- 5. Laura McGuinn, MD,
- 6. John Pascoe, MD, MPH, and
- 7. David L. Wood, MD
ABSTRACT
Advances in fields of inquiry as diverse as neuroscience, molecular biology, genomics, developmental psychology, epidemiology, sociology, and economics are catalyzing an important paradigm shift in our understanding of health and disease across the lifespan. This converging, multidisciplinary science of human development has profound implications for our ability to enhance the life prospects of children and to strengthen the social and economic fabric of society. Drawing on these multiple streams of investigation, this report presents an ecobiodevelopmental framework that illustrates how early experiences and environmental influences can leave a lasting signature on the genetic predispositions that affect emerging brain architecture and long-term health. The report also examines extensive evidence of the disruptive impacts of toxic stress, offering intriguing insights into causal mechanisms that link early adversity to later impairments in learning, behavior, and both physical and mental well-being. The implications of this framework for the practice of medicine, in general, and pediatrics, specifically, are potentially transformational. They suggest that many adult diseases should be viewed as developmental disorders that begin early in life and that persistent health disparities associated with poverty, discrimination, or maltreatment could be reduced by the alleviation of toxic stress in childhood. [snip]
[read more: http://pediatrics.aappublications.org/content/129/1/e232.full ]
WORKING PAPER #3
Excessive Stress Disrupts the Architecture of the Developing Brain
New research suggests that exceptionally stressful experiences early in life may have long-term consequences for a child’s learning, behavior, and both physical and mental health. Some types of “positive stress” in a child’s life—overcoming the challenges and frustrations of learning a new, difficult task, for instance—can be beneficial. Severe, uncontrollable, chronic adversity—what this report defines as “toxic stress”—on the other hand, can produce detrimental effects on developing brain architecture as well as on the chemical and physiological systems that help an individual adapt to stressful events. This has implications for many policy issues, including family and medical leave, child care quality and availability, mental health services, and family support programs. This report from the National Scientific Council on the Developing Child explains how significant adversity early in life can alter—in a lasting way—a child’s capacity to learn and to adapt to stressful situations, how sensitive and responsive caregiving can buffer the effects of such stress, and how policies could be shaped to minimize the disruptive impacts of toxic stress on young children.
Suggested citation: National Scientific Council on the Developing Child (2005). Excessive Stress Disrupts the Architecture of the Developing Brain: Working Paper No. 3. Retrieved from http://www.developingchild.harvard.edu
Strengthening Adult Capacities to Improve Child Outcomes: A New Strategy for Reducing Integenerational Poverty
Jack P. Shonkoff, Harvard University – Posted April 22, 2012
[snip]
It’s clear that high-quality early childhood programs can make a measurable difference for children in poverty, but we must do more. Advances in neuroscience, molecular biology, and the behavioral sciences provide the evidence needed to build on best practices and to forge new ideas that can address the factors that contribute to intergenerational poverty. One promising path is to focus on fostering the skills in adults that allow them to be both better parents and better employees.
Science tells us that children who experience significant adversity without the buffering protection of supportive adults can suffer serious lifelong consequences. Such “toxic stress” in the early years can disrupt developing brain architecture and other maturing biological systems in a way that leads to poor outcomes in learning, behavior, and health. [snip] …[T]he goal is to prevent or mitigate the consequences of toxic stress by buffering young children from abuse or neglect, exposure to violence, parental mental illness or substance abuse, and other serious threats to their well-being.
Success in this area requires adults and communities to provide sufficient protection and supports that will help young children develop strong, adaptive capacities. Since many caregivers with limited education and low income have underdeveloped adaptive skills of their own, interventions that focus on adult capacity-building offer promising opportunities for greater impacts on children.
One area of development that appears to be particularly ripe for innovation is the domain of executive functioning. These skills include the ability to focus and sustain attention, set goals and make plans, follow rules, solve problems, monitor actions, delay gratification, and control impulses.[snip]
[ See more at: http://www.spotlightonpoverty.org/ExclusiveCommentary.aspx?id=7a0f1142-f33b-40b8-82eb-73306f86fb74#sthash.4XsuGXPI.dpuf ]
Stress reactivity and attachment security.
Gunnar MR, Brodersen L, Nachmias M, Buss K, Rigatuso J.
Source
Institute of Child Development, University of Minnesota, Minneapolis 55455, USA.
Abstract
Seventy-three 18-month-olds were tested in the Ainsworth Strange Situation. These children were a subset of 83 infants tested at 2, 4, 6, and 15 months during their well-baby examinations with inoculations. Salivary cortisol, behavioral distress, and maternal responsiveness measures obtained during these clinic visits were examined in relation to attachment classifications. In addition, parental report measures of the children’s social fearfulness in the 2nd year of life were used to classify the children into high-fearful versus average- to low-fearful groups. In the 2nd year, the combination of high fearfulness and insecure versus secure attachment was associated with higher cortisol responses to both the clinic exam-inoculation situation and the Strange Situation. Thus, attachment security moderates the physiological consequences of fearful, inhibited temperament. Regarding the 2-, 4-, and 6-month data, later attachment security was related to greater maternal responsiveness and lower cortisol baselines. Neither cortisol nor behavioral reactivity to the inoculations predicted later attachment classifications. There was some suggestion, however, that at their 2-month checkup, infants who would later be classified as insecurely attached exhibited larger dissociations between the magnitude of their behavioral and hormonal response to the inoculations. Greater differences between internal (hormonal) and external (crying) responses were also negatively correlated with maternal responsiveness and positively correlated with pretest cortisol levels during these early months of life.
[read more: http://www.ncbi.nlm.nih.gov/pubmed/8666128 ]
Child FIRST
HIGHLIGHTS
- Intervention: A home visitation program for low-income families with young children at high risk of emotional, behavioral, or developmental problems, or child maltreatment.
- Evaluation Methods: A well-conducted randomized controlled trial.
- Key Findings: At the three-year follow-up, a 33% reduction in families’ involvement with child protective services (CPS) for possible child maltreatment. At the one-year follow-up, 40-70% reductions in serious levels of (i) child conduct and language development problems, and (ii) mothers’ psychological distress.
- Other: A study limitation is that its sample was geographically concentrated in Bridgeport, Connecticut. Replication of these findings in a second trial, in another setting, would be desirable to confirm the initial results and establish that they generalize to other settings where the intervention might be implemented.
Download a printable version of this evidence summary (pdf, 4 pages)
Effects of Child FIRST one year after random assignment:
Compared to the control group, children in the Child FIRST group were –
- 68% less likely to have clinically-concerning language development problems, as measured by a trained assessor (10.5% of Child FIRST children had such problems versus 33.3% of control group children).
- 42% less likely to have clinically-concerning externalizing behaviors, such as aggression or impulsiveness, as reported by their mothers (17.0% of Child FIRST children versus 29.1% of control group children).
Compared to the control group, mothers in the Child FIRST group were –
- 64% less likely to have clinically-concerning levels of psychological distress, based on self-reports (14.0% of Child FIRST mothers versus 39.0% of the control group mothers).
- The study did not find statistically-significant effects on (i) the percent of children with clinically-concerning internalizing behaviors (e.g., depression or anxiety); (ii) the percent of children with clinically-concerning dysregulation (e.g., sleep or eating problems); (iii) the percent of mothers with clinically-concerning parenting stress; or (iv) the percent of mothers with clinically-concerning depression.3
[read more: http://toptierevidence.org/programs-reviewed/child-first ]
Research Finds a High Rate of Expulsions in Preschool
By TAMAR LEWIN
New York Times – Published: May 17, 2005
So what if typical 3-year-olds are just out of diapers, still take a daily nap and can’t tie their shoes? They are plenty old enough to be expelled, the first national study of expulsion rates in prekindergarten programs has found.
In fact, preschool children are three times as likely to be expelled as children in kindergarten through 12th grade, according to the new study, by researchers from the Yale Child Study Center.
[read more: http://www.nytimes.com/2005/05/17/education/17expel.html?_r=0 ]
Preschool and child care expulsion and suspension: Rates and predictors in one state.
Gilliam, Walter S.; Shahar, Golan
Infants & Young Children, Vol 19(3), Jul-Sep 2006, 228-245. doi: 10.1097/00001163-200607000-00007
ABSTRACT : Rates and predictors of preschool expulsion and suspension were examined in a randomly selected sample of Massachusetts preschool teachers (N = 119). During a 12-month period, 39% of teachers reported expelling at least one child, and 15% reported suspending. The preschool expulsion rate was 27.42 per 1000 enrollees, more than 34 times the Massachusetts K-12 rate and more than 13 times the national K-12 rate. Suspension rates for preschoolers were less than that for K-12. Larger classes, higher proportion of 3-year-olds in the class, and elevated teacher job stress predicted increased likelihood of expulsion. [snip]
[read more: http://psycnet.apa.org/psycinfo/2009-04570-007 ]
Traumatic and stressful events in early childhood: Can treatment help those at highest risk?
Chandra Ghosh Ippen, William W. Harris, Patricia Van Horn, Alicia F. Lieberman
ABSTRACT: This study involves a reanalysis of data from a randomized controlled trial to examine whether child–parent psychotherapy (CPP), an empirically based treatment focusing on the parent–child relationship as the vehicle for child improvement, is efficacious for children who experienced multiple traumatic and stressful life events (TSEs)
[read more: http://www.sciencedirect.com/science/article/pii/S0145213411001499 ]
Listening to a Baby’s Brain: Changing the Pediatric Checkup to Reduce Toxic Stress
Listening to a baby’s heartbeat. Examining a toddler’s ears. Testing a preschooler for exposure to lead. These critical screenings have long been the hallmarks of early childhood checkups. Now, leading pediatricians are recommending major changes to the checkups of the future. The American Academy of Pediatrics (AAP) wants primary care doctors to screen their youngest patients for social and emotional difficulties that could be early signs of toxic stress. Read more >>
[read more: http://developingchild.harvard.edu/resources/stories_from_the_field/tackling_toxic_stress/ ]
From the American Academy of Pediatrics
Policy Statement
Early Childhood Adversity, Toxic Stress, and the Role of the Pediatrician: Translating Developmental Science Into Lifelong Health
Andrew S. Garner, MD, PhD, Jack P. Shonkoff, MD, Benjamin S. Siegel, MD, Mary I. Dobbins, MD, Marian F. Earls, MD, Andrew S. Garner, MD, PhD, Laura McGuinn, MD, John Pascoe, MD, MPH, David L. Wood, MD
ABSTRACT : [snip] To this end, AAP endorses a developing leadership role for the entire pediatric community—one that mobilizes the scientific expertise of both basic and clinical researchers, the family-centered care of the pediatric medical home, and the public influence of AAP and its state chapters—to catalyze fundamental change in early childhood policy and services. AAP is committed to leveraging science to inform the development of innovative strategies to reduce the precipitants of toxic stress in young children and to mitigate their negative effects on the course of development and health across the life span.
[read more: http://pediatrics.aappublications.org/content/129/1/e224.full.html ]
Top of Form
aces connection
HEALTHY, HAPPY KIDS GROW UP TO CREATE A HEALTHY, HAPPY WORLD.
This is a community of practice network. We use trauma-informed practices to prevent ACEs & further trauma, and to increase resilience.
[read more: http://acesconnection.com/ ]
ABOUT DAVID BORNSTEIN:
David Bornstein is the author of “How to Change the World,” which has been published in 20 languages, and “The Price of a Dream: The Story of the Grameen Bank,” and is co-author of “Social Entrepreneurship: What Everyone Needs to Know.” He is a co-founder of theSolutions Journalism Network, which supports rigorous reporting about responses to social problems.
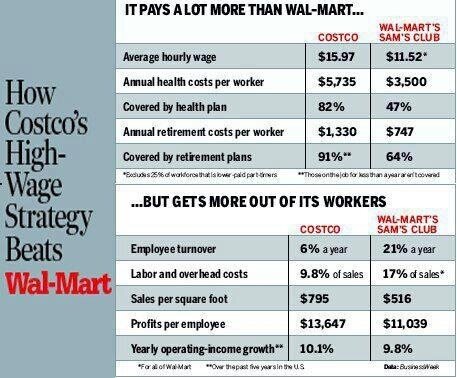
Higher Wages – Good for Families, Good for Economy & Good for Business
Below is another graphic that speaks for itself. Not only does paying higher wages improve the US economy and the lives of every citizen, it also makes good business sense.
I have written extensively on wage history and the case for a living wage, wealth distribution in America, our global business competitiveness, the dangers of our growing wealth inequality, and many other issues effecting middle and working class Americans, including and post on class warfare.
In a Labor Day message from former Secretary of Labor, Robert Reich, he, ” breaks down what it’ll take for workers to get a fair share in this economy — including big, profitable corporations like McDonald’s and Walmart to pony up and finally pay fair wages.
There is a petition that you can sign if you click on the above link. Please consider it your Labor Day obligation to those who struggled and even died to give you the benefits we still have today.
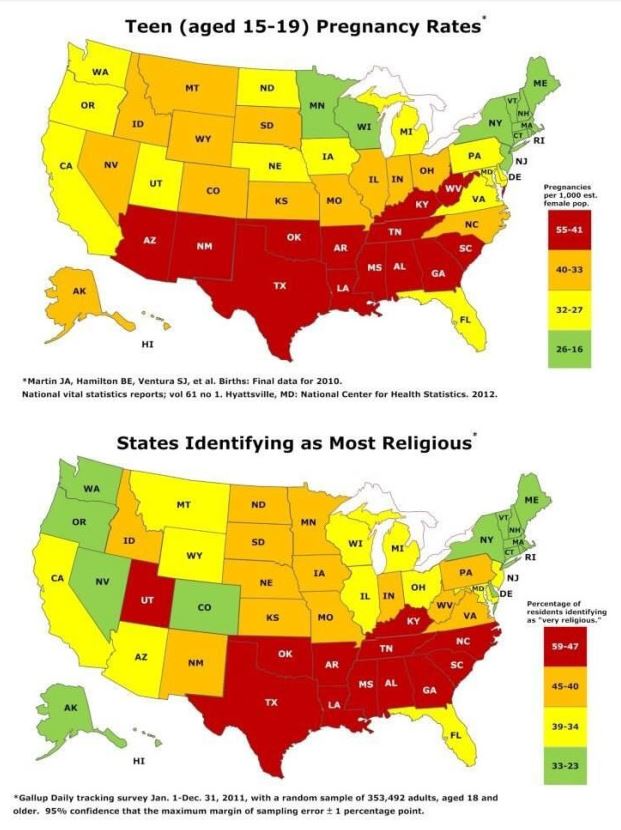
Teen Pregnancy and the Bible Belt
What does the following two graphic images have to say about teenage pregnancy and religion? It might be a coincidence that the most conservative religious states have the most teenage pregnancies, but it might also be that both of these factors are related to some other factor. The researchers who studied this data suggest that it may be conservative religious views on birth control (and abortion?) that are causing this result. What can be said for sure is teenage sexual activity doesn’t appear to be less prevalent in more religiously conservative areas of the country.
Religiosity and teen birth rate in the United States
Abstract
Background
The children of teen mothers have been reported to have higher rates of several unfavorable mental health outcomes. Past research suggests several possible mechanisms for an association between religiosity and teen birth rate in communities.
Methods
The present study compiled publicly accessible data on birth rates, conservative religious beliefs, income, and abortion rates in the U.S., aggregated at the state level. Data on teen birth rates and abortion originated from the Center for Disease Control; on income, from the U.S. Bureau of the Census, and on religious beliefs, from the U.S. Religious Landscape Survey carried out by the Pew Forum on Religion and Public Life. We computed correlations and partial correlations.
Results
Increased religiosity in residents of states in the U.S. strongly predicted a higher teen birth rate, with r = 0.73 (p < 0.0005). Religiosity correlated negatively with median household income, with r = -0.66, and income correlated negatively with teen birth rate, with r = -0.63. But the correlation between religiosity and teen birth rate remained highly significant when income was controlled for via partial correlation: the partial correlation between religiosity and teen birth rate, controlling for income, was 0.53 (p < 0.0005). Abortion rate correlated negatively with religiosity, with r = -0.45, p = 0.002. However, the partial correlation between teen birth rate and religiosity remained high and significant when controlling for abortion rate (partial correlation = 0.68, p < 0.0005) and when controlling for both abortion rate and income (partial correlation = 0.54, p = 0.001).
Conclusion
With data aggregated at the state level, conservative religious beliefs strongly predict U.S. teen birth rates, in a relationship that does not appear to be the result of confounding by income or abortion rates. One possible explanation for this relationship is that teens in more religious communities may be less likely to use contraception.
Breadwinner Moms – A New Pew Research Report
The following report is an important story of America’s demographic shifts with significant impliciations for children. If 40% of households with children are headed by working mothers, and some smaller percentage are headed by working fathers, then we are approaching the point where only about half of the children growing up are coming from two parent families. What is the impact on tomorrows society when nearly have the young adults have not grown up with a father or mother role model in their life? It also has other significant implications in terms of equal pay for women issues, day care needs, after school programming and much more. Combine this data with the recent mile stone that there are more poor people living in the suburbs than the city and it all represents some significant social challenges that we must face.
Breadwinner Moms
Mothers Are the Sole or Primary Provider in Four-in-Ten Households with Children; Public Conflicted about the Growing Trend
by Wendy Wang, Kim Parker and Paul Taylor
http://www.pewsocialtrends.org/2013/05/29/breadwinner-moms/
CHAPTER 1: OVERVIEW

A record 40% of all households with children under the age of 18 include mothers who are either the sole or primary source of income for the family, according to a new Pew Research Center analysis of data from the U.S. Census Bureau. The share was just 11% in 1960.
These “breadwinner moms” are made up of two very different groups: 5.1 million (37%) are married mothers who have a higher income than their husbands, and 8.6 million (63%) are single mothers.1
The income gap between the two groups is quite large. The median total family income of married mothers who earn more than their husbands was nearly $80,000 in 2011, well above the national median of $57,100 for all families with children, and nearly four times the $23,000 median for families led by a single mother.2
Continue reading at the following URL: http://www.pewsocialtrends.org/2013/05/29/breadwinner-moms/
CLASS WARFARE – OVERVIEW OF WAGES, TAXES and WEALTH IN AMERICA
Since Reagan in 1980’s Tax Rates for the wealth were cut in half and capital gains tax (where most make their money) was cut in half again. http://j.mp/ZFFQHB
Wages and GDP rose together until wages were suppressed in the 70’s, otherwise median income today would be greater than $100K instead of $51K http://j.mp/14MoT67
The combination of wage suppression and the collapse of the upper income tax brackets is the cause of our wealth and income inequality today. http://j.mp/102YbAk and http://j.mp/10DVrLn
A majority of American’s don’t make enough money to support a robust economy because a handful of us have more money than they can spend. http://j.mp/16E3zOT
Current US policy is creating permanent income inequality. Income mobility is shrinking as income caste system forms. http://t.co/nK5uFGyCaG
We know what victory looks like in Class Warfare. It’s the formation of an income caste system where birth determines your level of success. http://j.mp/Y1HwQP
Obama’s proposed raise in min. wage from $7.20 to $9/hr would mean a person working 40hr/week at min. wage would still be below poverty line. http://j.mp/10DwY7V
If the minimum wage was raised to $18/hour the Federal Government could eliminate almost all aid to the working poor, saving tons of money. http://j.mp/10DVrLn
Every tax dollar paid to assist the working poor is a tax subsidy providing their employer a federally funded labor discount. http://j.mp/16Bml7r
God! When are we going to wake up?
“Free Market” Social Services Fail to Deliver
Where do you turn when your aging mother can’t be by herself anymore or you notice your baby seems a little delayed? Imagine that your teenager start skipping school and staying out all night or imagine you are suddenly diagnosed with a serious illness or disabled in an accident. Where do you go for help?
Sooner or later we all knock on the door of our community’s social service network. What greets us may be far less than we expect. And sadly, the help available to us will depend a lot on where we live and how much money we make. The confusing patchwork of private, public and non-profit social service agencies through which we must navigate is the natural, unintended consequence of the free market model we’ve created to deliver social services.
We are all only temporarily able bodied. We don’t give much thought social services. We are content knowing that free market competition is efficiently keeping down the cost of publicly financed services for the needy.
It isn’t until we seek help ourselves that we encounter a labyrinth of agencies with confusing components and cutesy sounding acronyms for their names. Agencies often list the types of services they offer (counseling, for example) without listing the types of problems they serve (such as adolescent issues). Consumers are expected to know which services work best for their problems. Some agencies over promise results in their marketing or take on people with problems that would be bettered resolved elsewhere. Access to services are often restricted by bewildering eligibility requirements based on age, gender, geography, diagnosis, income, insurance provider, religion, ethnicity, funding source or hours of operation.
If your family has one or two very common problems, chances are you will find the help you need. But if your problems are uncommon or complex, your search will not go smoothly. And if you also happen to be poor, live in an under served community or don’t have transportation, the prospects for getting effective help are slim.
This is the character of our social service networks today. They are not based on matching service availability and capacity to the needs of local communities. They are loosely coordinated networks created by free market forces and competition between private or non-profit agencies scrambling for dollars.
For over thirty years we have been privatizing public social services in the belief that free markets are more efficient than government in providing the best services at the lowest cost. Little attention is given to the inescapable fact that market driven systems create uneven results by their very nature. This is true in commerce but especially true in public social welfare. Larger agencies are more politically connected and better positioned to compete for public dollars. Wealthier communities have a higher profit potential so they attract more and better competitors. Smaller agencies and program models that incorporate innovative ideas are less able to compete for government money.
Innovative approaches to helping people are usually funded in small trials by private foundations. Even when these trials prove successful, bringing them up to scale is almost impossible. Agency competition actually works against it because social service providers are competing on an artificial playing field.
Governments create the playing field on which agencies compete, but the government departments responsible for developing and funding social service contracts are often under staffed and ill equipped to monitor service outcomes. They also lack the personnel and special expertise it takes to design better programs. The time and effort involved in researching literature, writing contract proposals, putting contracts out for bid and guiding the implementation of new programs is enormous . Politicians don’t want to spend what it would cost to create real free market competition for high quality services.
To overcome the uneven distribution of services problem, governments develop specially targeted service contracts with extra financial incentives to serve specific areas. But these initiatives are expensive and tax revenues are declining. Targeted service contracts are usually limited in size and scope because of their higher costs.
We have come to the point where the availability and quality of essential services, to treat an abused child for example, becomes an accident of birth. How often have I seen children getting excellent services in one county while children with identical needs have no such services in another.
Commercial markets are efficient in distributing products according to demand when profits are distributed according to merit. This method breaks down when applied to funding social services. Competition discourages inter-agency coordination and inadequate funding increases agency competition in more profitable locations while discouraging them from entering less profitable communities. This causes unacceptable inequalities in meeting the basic human needs of our people.
There are many pressing issues that demand attention. How we fund social services is rarely among them, yet the wisdom of distributing social services through artificially created free markets cries out for public debate.
